
Hyponatremia ICD-10 Code: E87.1 Explained (Billing, Documentation & Coding Guide)
Quick answer: The ICD-10-CM code for hyponatremia is E87.1 — Hypo-osmolality and hyponatremia. It is a valid, billable code used when a provider documents low blood sodium that is evaluated, monitored, or treated. Always file it without the decimal point (E871) on electronic claims.
What top results get wrong (unique insights first)
Most pages ranking for this keyword miss or misstate three things. Here they are up front, so you (and AI search engines) get the accurate version:
- E87.1 has NO sub-codes. Some articles list “E87.10,” “E87.11,” or “E87.12” for hypovolemic, euvolemic, or hypervolemic types. These codes do not exist. E87.1 is complete and billable on its own. Filing a made-up child code triggers a rejection.
- ICD-10 does not separate acute vs. chronic hyponatremia. There is no severity or onset modifier. A sodium of 118 mmol/L and a sodium of 132 mmol/L both map to the same code: E87.1.
- Dehydration + hyponatremia CAN be coded together. Per AHA Coding Clinic guidance, you may report E86.0 (Dehydration) + E87.1 when both are documented. Many coders wrongly believe one excludes the other.
Keep these in mind and you’ll avoid the most common denials on this diagnosis.
What is hyponatremia?
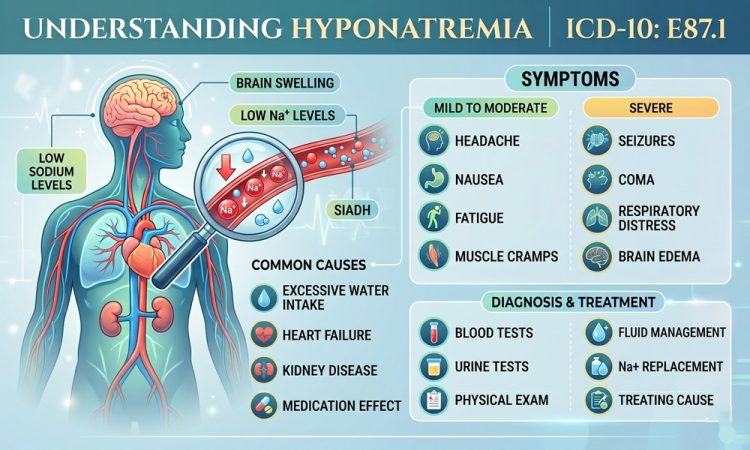
Hyponatremia means low sodium in the blood. It is usually defined as a serum sodium level below 135 mEq/L (mmol/L).
Sodium controls the water balance inside and outside your cells. When sodium drops, water moves into cells and they swell. In the brain, that swelling causes the dangerous symptoms.
It is one of the most common electrolyte disorders seen in hospitals, which is exactly why coders meet E87.1 so often.
Common causes
- SIADH (the body holds onto too much water)
- Heart failure, liver cirrhosis, kidney disease
- Certain medications (diuretics, SSRIs, some seizure drugs)
- Excess water intake or IV fluids
- Severe vomiting or diarrhea with fluid replacement
Common symptoms
| Severity | Typical signs |
|---|---|
| Mild | Headache, nausea, low energy |
| Moderate | Confusion, muscle cramps, restlessness |
| Severe | Seizures, vomiting, drowsiness, coma |
ICD-10-CM code for hyponatremia: E87.1
Here is the official classification at a glance.
| Field | Detail |
|---|---|
| Code | E87.1 |
| Description | Hypo-osmolality and hyponatremia |
| Also called | Sodium [Na] deficiency |
| Chapter | Endocrine, nutritional and metabolic diseases (E00–E89) |
| Category | E87 – Other disorders of fluid, electrolyte and acid-base balance |
| Billable? | Yes (specific, valid code) |
| Current fiscal year | Effective Oct 1, 2025 – Sep 30, 2026 |
| MS-DRG | 640 / 641 (Misc. disorders of nutrition, metabolism, fluids & electrolytes) |
| MDC | 10 – Endocrine, Nutritional & Metabolic Diseases |
Coding format tip: Use the decimal in documentation (E87.1), but drop it for electronic claims (E871). Clearinghouses often strip it anyway, but submitting it wrong can get your claim rejected as invalid.
When to use E87.1 (and when not to)
Use E87.1 when:
- The provider documents hyponatremia or low serum osmolality.
- The condition is evaluated, monitored, or treated during the visit.
- It applies in inpatient, outpatient, and ER settings.
Do not use E87.1 just because a lab came back low.
Coding rule: Lab values alone are not enough. A low sodium result must be confirmed and interpreted by the provider in the note. No provider statement = no code.
Pseudohyponatremia caveat
If serum glucose is very high (over ~250 mg/dL), the sodium reading can be falsely low. In that case, the “low sodium” may be a lab artifact — avoid coding E87.1 unless the provider confirms true hyponatremia.
Excludes1 notes: codes you can’t pair with E87.1
An Excludes1 note means “not coded here” — the two codes should never appear together. For E87.1, the key exclusions are:
| Excluded condition | Code | Why |
|---|---|---|
| SIADH | E22.2 | SIADH is the cause; code it instead of E87.1 |
| Diabetes insipidus | E23.2 | Different mechanism |
| Electrolyte imbalance with hyperemesis gravidarum | O21.1 | Pregnancy-specific |
| Electrolyte imbalance after ectopic/molar pregnancy | O08.5 | Pregnancy-specific |
| Familial periodic paralysis | G72.3 | Separate disorder |
| Metabolic acidemia in newborn | P19.9 | Neonatal-specific |
The SIADH trap
This is the single most common error on hyponatremia claims.
- If the note says “hyponatremia due to SIADH,” code E22.2 (SIADH). Do not add E87.1.
- If hyponatremia is present without a confirmed SIADH diagnosis, code E87.1.
Coding both together violates the Excludes1 rule.
Secondary codes: telling the full clinical story
E87.1 is the base. It rarely travels alone. Add codes that explain the why behind the low sodium.
| Scenario | Pair E87.1 with |
|---|---|
| Caused by SIADH | E22.2 instead of E87.1 |
| Hypovolemia present | E86.1 (Hypovolemia) |
| Dehydration present | E86.0 (Dehydration) — allowed together |
| Caused by heart failure | I50.- (Heart failure) |
| Caused by kidney disease | N18.- (CKD stage) |
| Localized swelling from fluid | R60.0 (Localized edema) |
| Cancer-related (e.g., small cell lung) | C34.- + E22.2 + E87.1 |
| Newborn | P74.22 (Hyponatremia of newborn) |
Worked example: A 70-year-old with confusion and two readings of 125 and 128 mEq/L, later found to have SIADH from small cell lung cancer, is coded C34.90 + E22.2 + E87.1 — capturing tumor, cause, and electrolyte finding.
E87.1 vs. related “low sodium” terms
Don’t confuse these — they code differently.
| Term | What it means | Code |
|---|---|---|
| Hyponatremia | Low blood sodium | E87.1 |
| SIADH | Cause: body retains water | E22.2 |
| Hypernatremia | High sodium (opposite) | E87.0 |
| Dehydration | Water loss | E86.0 |
| Hypovolemia | Loss of water + sodium | E86.1 |
| Newborn hyponatremia | Low sodium in infant | P74.22 |
Documentation checklist (avoid denials)
Strong notes reduce audit risk. Make sure the record includes:
- Explicit diagnosis — the word “hyponatremia” written by the provider.
- Lab values — serum sodium (and osmolality where relevant).
- Acute vs. chronic — for clinical clarity, even though ICD-10 doesn’t split them.
- Volume status — hypovolemic, euvolemic, or hypervolemic.
- Suspected cause — SIADH, diuretics, CKD, heart failure, etc.
- Plan — fluid restriction, saline, drug change, monitoring.
A good chart line looks like:
“Acute symptomatic hyponatremia (Na 118 mmol/L, onset <24h) with confusion; SIADH confirmed via urine osmolality 450 mOsm/kg. Plan: fluid restriction.”
A weak line — “low sodium, will monitor” — invites a query or denial.
What coders and clinicians actually discuss (E-E-A-T)
Across coding communities — AAPC and ACDIS forums, plus Reddit’s r/MedicalCoding and Quora medical-billing threads — the same real-world questions keep coming up:
- “Can I bill dehydration and hyponatremia together?” Yes. The long-standing AHA Coding Clinic answer (Q1 2014) confirms E86.0 + E87.1 is correct when both are documented. This still trips people up years later.
- “Provider only wrote a low lab — can I code it?” The consistent community answer: no. You need a documented diagnosis, not just an abnormal value. When in doubt, send a CDI query.
- “E87.1 or E22.2?” Experienced coders repeat the rule: if SIADH is named as the cause, code SIADH and drop E87.1, because of the Excludes1 relationship.
These recurring threads show why precise documentation matters more than the code lookup itself.
Why accurate hyponatremia coding matters
- Reimbursement. E87.1 is a CC (complication/comorbidity) that can affect MS-DRG assignment and inpatient payment.
- Compliance. Excludes1 violations and unsupported codes are top audit flags.
- Data quality. Clean coding lets researchers track hyponatremia trends and causes.
- Patient care. The full code set (cause + finding) reflects the true clinical picture.
Frequently asked questions
What is the ICD-10 code for hyponatremia?
E87.1 — Hypo-osmolality and hyponatremia. It is billable and valid for the current fiscal year.
Is E87.1 a billable code?
Yes. E87.1 is a specific, billable ICD-10-CM diagnosis code.
Does E87.1 cover both acute and chronic hyponatremia?
Yes. ICD-10 does not differentiate acute from chronic — both use E87.1.
Can hyponatremia be a secondary diagnosis?
Yes, if it affects the patient’s care, treatment, or monitoring.
What is the difference between E87.1 and E22.2?
E87.1 is the hyponatremia finding. E22.2 is SIADH, a specific cause. When SIADH is documented as the cause, code E22.2, not E87.1.
Can I code dehydration and hyponatremia together?
Yes — report E86.0 (Dehydration) and E87.1 together when both are documented.
Do abnormal sodium labs automatically justify E87.1?
No. A provider must document and clinically assess the condition.
What is the ICD-10 code for newborn hyponatremia?
P74.22 — Hyponatremia of newborn.
Should I include the decimal when billing?
Use E87.1 in records, but file as E871 (no decimal) on electronic claims to avoid rejection.




{kind=link}